



Why is it that, in spite of mounting pressure from parents, private clinics, and the press, the plagiocephaly NHS stance isn’t changing? This guide covers everything you need to know about the matter.
NHS Flat Head Advice
For positional plagiocephaly the NHS website advises that a baby’s skull ‘should correct itself naturally over time’ if simple measures to take pressure off the flattened area are carried out, encouraging parents to reposition their baby. Essentially when it comes to plagiocephaly and brachycephaly, flat head NHS guidelines point to repositioning as the blanket solution.
Here is the plagiocephaly NHS advice as stated on their website:
“There are specially designed helmets and headbands that some people claim can help improve the shape of a baby’s skull as they grow.
These devices apply pressure to “bulging” parts of the skull and relieve pressure from other parts, potentially allowing growth in the flatter areas.
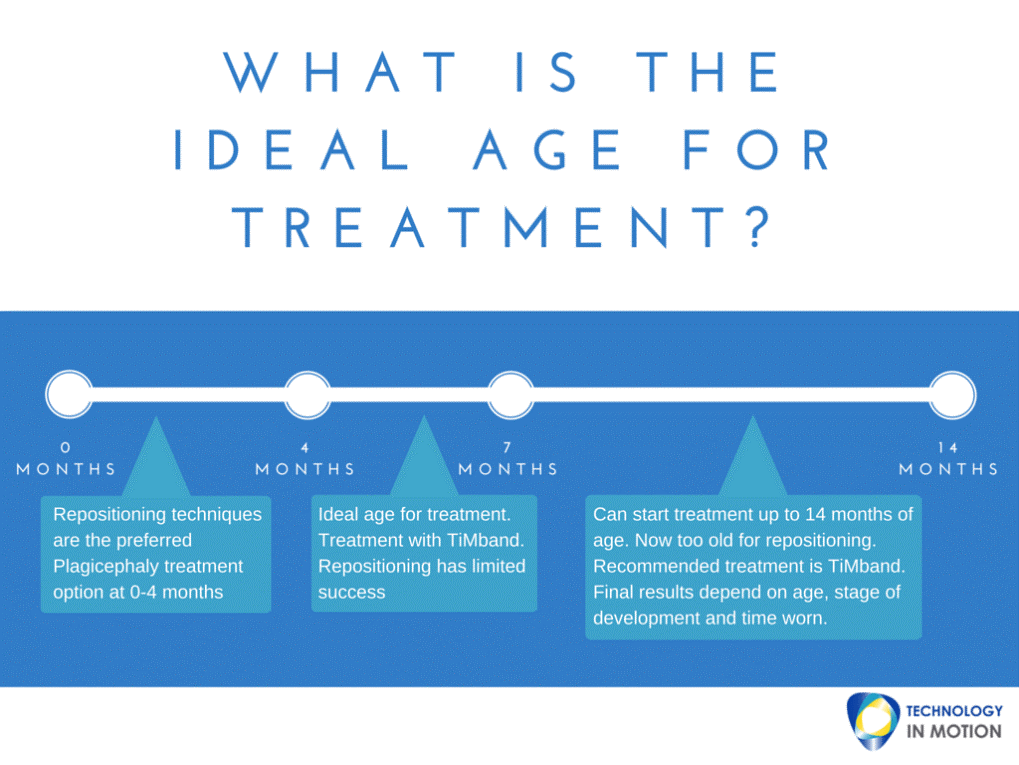
Treatment is started when the child’s skull is still soft, usually at around 5 or 6 months old, and the device is worn almost continuously (up to 23 hours a day) for several months.
But these helmets and headbands generally aren’t recommended because:
- There isn’t clear evidence to suggest they work
- They often cause problems such as skin irritation and rashes
- They’re expensive, typically costing around £2,000
- Your baby will need to be checked every few weeks to monitor their head growth and make any necessary adjustments
- They may be uncomfortable and distressing for your baby”
And
- “You may consider using a helmet or headband if you’re worried about your child, but it’s not clear whether these always work. You should also bear in mind the inconvenience, expense and possible discomfort for you and your child.”
Another recent study published in The Journal of Craniofacial Surgery (January 2014) looked at rates of parent satisfaction concerning the therapy and concluded that:
“More parents who used helmet therapy reported that they were satisfied with their child’s long-term head shape and would choose the same treatment again compared with those who used repositioning therapy.”
In spite of a wealth of convincing evidence, mounting pressure from the press and countless case studies, the NHS’s stance against remoulding therapy has become even firmer. Faced with this paradox, we have decided to start our campaign, challenging the NHS to advise that cranial helmets are the standard treatment for severe plagiocephaly. While we recognise that the NHS has difficulties with funding, we believe that this should not prevent them from providing parents with clinically sound advice.
It certainly is true that, if parents try active repositioning from the very first moment that a deformity is noticed, plagiocephaly is likely to correct. However, this isn’t the case for all babies.
Where Did the NHS Flat Head Advice Come From?
The NHS has based their advice and policies regarding flat head syndrome, which is not to provide therapy on the basis of one single piece of research by Renska Van Wijk. Published in 2014, Renska was researching for her PhD at the time, she concluded at the end of the study the change found in a group of babies who had helmet therapy and those that didn’t, were equal. Therefore, concluding helmet therapy should be discouraged as a standard treatment for healthy infants with moderate to severe skull deformation.
However, there are a few significant factors which need to be considered with this study. Firstly, this ‘open source’ paper was funded on the premise that the research data is freely available for other researchers to access, however, the author has since denied access to her data.
On examination, the study was looking for 200 infants to be assigned to a treated and a non treated group and 403 infants were chosen. Of these only 84 parents agreed to allow their infants to be entered into the trial, 42 for each group.
Of the ‘treated’ group, only 30 were actually provided with helmet treatment as some parents decided not to take up treatment. 22 parents reported problems with the fitting of the helmet and 20 abandoned treatment before the predicted end of treatment. Leaving 10 infants in the fully treated group.
These 10 infants were treated across 4 locations using two different types of helmet and this eventually became essentially a minimal patient case study. It’s worth noting that one of the manufacturers immediately stopped providing their product on the release of the report. It’s not surprising therefore to note that the two groups, treated and non-treated, demonstrated a similar result. These helmets were labelled as ‘ineffective’, however, the treatment process and the helmets used in the report were not monitored.
For Technology in Motion, the report has one critical conclusion. Up until the age of 24 months, moderate head shapes will naturally improve, but only marginally (2.6% for plagiocephaly and 5.4% brachycephaly). Whilst this is encouraging for parents, this is not nearly enough to correct the severely deformed head shapes that we regularly see at our clinics.
The report also notes that 75% of the infants that took part in the study continued to have a persistent skull shape deformity. The NHS seems fixated on the fact that there was an equal measure of change between the two groups, during the time period of the study, using it as justification by stating there isn’t clear evidence to indicate helmet therapy works. Yet they fail to take into consideration that an astonishing 75% of these infants still had skull deformities, having the option of helmet therapy taken away from them, as they have surpassed the age of when treatment is effective.
Evidence Opposing the NHS Flat Head Syndrome Stance
For brachycephaly specifically, a paper published in 2018 titled Helmet Treatment of Infants with Deformational Brachycephaly, concluded that cranial orthosis is successful in the correction of deformational brachycephaly. It also demonstrated that entrance age for cranial remoulding therapy is a critical variable in the overall effectiveness of treatment, with younger infants demonstrating both improved outcomes and shorter treatment times. This supports our advice to parents, explaining why there is an optimal age and a specific window in an infant’s early life to undergo treatment. This evidence overall determines that helmet therapy can be used to effectively and successfully treat brachycephaly, as well as plagiocephaly.
Moreover, there is specific data which shows what percentage of infants will go on to have a severely deformed head shape if treatment isn’t pursued. These statistics are shown across two studies which are linked. The first paper follows infants in the first two years of life in relation to the development of brachycephaly and plagiocephaly. The follow-up paper then revisits the participants at ages 3-4. The standout conclusion from both of these papers, for us particularly, is that 3-4% (1 in 25 infants of the population) who have a severe head shape at 2 will still have a severely deformed head shape at age 3 and 4. Thus, demonstrating that not all cases of flat head syndrome will correct itself and in terms of the whole population of infants, 1 in 25 is a considerable amount.
Another study, published in the British Medical Journal (2010), followed up on babies aged 3-4 years who had been previously diagnosed with deformational plagiocephaly and whose parents had been fully counselled on repositioning.
The researchers found that 61% of head shape measurements had reverted to within the normal range, while most of the remainder had shown ‘good improvement’. However, 13% demonstrated ‘poor improvement’, of whom 4% remained with ‘severe’ plagiocephaly. Accordingly, 13% of parents remained ‘somewhat’ or ‘very’ concerned at follow-up.
From this, it is clear that, in some cases, plagiocephaly does not self-correct, even with active repositioning. It is this 4% of the population that plagiocephaly helmets are designed for. Some cases of plagiocephaly are too severe for simple repositioning to have a significant effect.

Why Can’t Parents Get a Plagiocephaly Helmet on the NHS?
To the NHS, flat head syndrome is seen as ‘only cosmetic’
The most common reason given by the health system for their refusal to fund reshaping is that positional plagiocephaly is ‘just’ or ‘only’ cosmetic. However, it is important to note that young children are especially vulnerable to psychosocial trauma as a result of bullying and social exclusion, as explained in our guide on The Long Term Effects of Plagiocephaly.
The NHS believes plagiocephaly can be covered by hair
The NHS states that “as your child becomes more mobile and their hair grows, the appearance of their head should improve. It’s very rare for a child to experience problems such as teasing when they reach school age“.
As a result, many parents have been calling for the NHS to review their priorities, as looking at hair growth as a ‘cover-up’ solution to plagiocephaly is dismissive to the long-term effects of living with plagiocephaly and how it can affect a child later in life. Not all children, and indeed when grown into adults, have enough hair to cover up a misshapen head, so relying on this as a solution is poor.
Stockton-on-Tees mother, Melanie Grayson, decided to take her 5 month-old son, Charlie, to a private plagiocephaly clinic, “rather than take the risk that his head may get better and look OK with hair'”, she told Gazette Live at the time.
“The use of helmets and headbands is controversial”
Two years ago, an article about baby Coby, the son of one of our clients, was published in the Daily Mail. Included in the article was a list of ‘downsides’ to helmets according to the NHS. This sparked national debate and we gave our response, a summary of which is provided below.
Will Parents Ever Have Access to NHS Flat Head Treatment?
The advice on the NHS website has been updated regarding plagiocephaly support, perhaps in response to pressure for it to change its stance. They now acknowledge that helmets can be an effective treatment for plagiocephaly, however, the tone is still disparaging as they claim that there isn’t clear evidence to suggest they work.
However, we see on a daily basis how effective plagiocephaly remoulding is as a treatment. In 2015, the largest study of its kind was published, which researched the effectiveness of helmet therapy for positional cranial deformation. The study of which was overwhelming, with complete correction being successfully achieved in 94.4% of patients treated with helmet treatment as first-line therapy. Additionally, 96.1% of infants who received helmets after failed repositioning techniques also achieved complete correction. Take a look at our research page for more research into plagiocephaly and reshaping therapy.
As we have seen, there is an overwhelming body of evidence indicating that helmets are an effective treatment for plagiocephaly. However, it looks as though we still have a way to go until parents have access to NHS-funded therapy.
To return to the original question of why you can’t get a plagiocephaly helmet on the NHS, the answer might not be so straightforward. While the NHS acknowledges plagiocephaly and brachycephaly, in spite of frequent attention from the press, mounting pressure from the public, and even scientific evidence, the NHS still refuses to fund treatment.
Our Mission to Get Funded Support from the NHS
We are incredibly grateful to all parents for helping us to spread the word, and ask that you continue to rally together to help end the NHS flat head stigma. Children who are not treated face living with a permanent deformity that could otherwise have been corrected, and we regularly receive calls from the parents of children and young adults asking if we can help them. Unfortunately, we can’t. The only option in these cases is open skull surgery.
There is immense strength in numbers, and the positive stories that you kindly share with us on Facebook and Instagram are a heartfelt testament to the importance of this cause. So keep sharing your experiences with other parents! Let’s not stop pushing until all the parents who need it have access to plagiocephaly treatment on the NHS, or at the very least, sound, clinically based information on the options that are available to them.
In the meantime, if you have a baby with severe plagiocephaly, Technology in Motion can help. Our TiMbandAir treatment is safe, pain-free and highly effective, and while it might not yet be available on the NHS, several charities can help you raise funds if required. Call us on 0330 100 1800, and we will arrange an appointment with one of our clinicians.
Here at Technology in Motion, we offer a free, no-obligation evaluation to assess the severity of the deformity. Should treatment be recommended, we provide sound, research-backed advice in every individual assessment.
Call 0330 100 1800 to arrange an appointment or browse our website for more information on our clinics and the services that we provide.





