



What is craniosynostosis?
The term "craniosynostosis" consists of three components:
- Cranio: relating to the skull,
- Syno: meaning together,
- Stosis: meaning relating to bones.
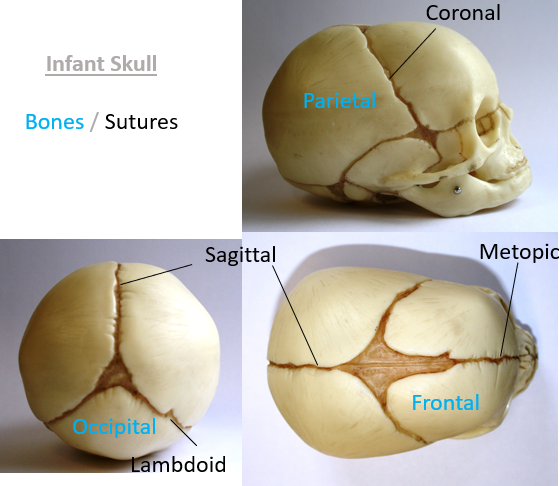
At birth, we possess malleable bones that can be shaped during delivery. The skull is composed of pliable, soft bones connected by fibrous seams called sutures. These sutures allow the skull to remain flexible, accommodating the growing brain and facial development as we age. The broader spaces where three or four bones meet are known as fontanelles, which typically close within the first few years of life.
However, in cases of craniosynostosis, one or more sutures close or "fuse" prematurely, often leading to unexpected complications as the baby undergoes growth.
As we grow all of our bones remain flexible, each with its own growth plate or growth areas to allow the skeleton to develop normally. In the long bones of the arms and the legs these plates are close to one end of the bone. In the wide flat bones, such as the bones of the skull the fibrous sutures do this work allowing the bones to gradually separate so that the brain can grow.
Sometimes, these growth areas don’t work properly and they can fuse before they should. This is what happens in craniosynostosis.
If one of the sutures is prematurely closed the head can’t grow as it should in that area, causing deformity and potential increase in pressure on the growing brain.
So what causes craniosynostosis?
Really, the causes of craniosynostosis in most infants are unknown. About 20% of infants have a genetic source which can result in syndromes such as Pfeifer, Crouzon, or Apert syndrome. All of which are rare.
Most cases are thought to be caused by several factors such as a single gene code combined with something that the mother encounters in her environment, such as medications, foods or drinks or underlying maternal health challenges during pregnancy.
If it’s not been picked up by the pre-birth scans a synostosis is usually, but not always picked up immediately after the birth. Sometimes it can be missed and it’s diagnosed later in life.
The first signs can be a misshapen skull and craniosynostosis can be confused with deformational plagiocephaly. The shape that is seen in clinic is very different in a plagiocephaly than a synostosis and it’s immediately obvious which type of condition it is and this can be confirmed by simple measurements.
Every baby who is born with craniosynostosis is different and it can be a severe or mild condition and most babies with the condition are otherwise healthy. In some children there can be some reported development delay issues either because the craniosynostosis has delayed m=normal brain growth or development or because of an underlying genetic condition and an infant who has had a craniosynostosis might need help throughout childhood to make sure that the brain and skull are developing properly.
Other indicators of craniosynostosis can be an absent fontanelle (soft spot); a raised bony line under the skin where the suture has closed, slow head growth, a lethargic baby or one which suddenly cries out as if in pain.
If a clinician or doctor suspects a synostosis the first test that can be used to confirm this is an x-ray or CT scan which shows the underlying structures of the skull.
Types of craniosynostosis
The common types of synostosis occur in the higher part of the skull, this area is called the skull vault and this area protects the brain.
- Sagittal Suture: This is the most common type of craniosynostosis and it stops the head from growing in width. So a long thin head shape, often with an over developed brow and occiput is the result.
- Uni-coronal Suture: This is the coronal suture on one side of the head. The eye on the affected side tends to be more open and the brow and face is flattened on this side, the bridge of the nose can be pulled across and the ear on the affected side can also be pulled forward.
- Bi-coronal Suture: Both coronal sutures are closed. The head can’t grow front to back so can be become very tall with a high forehead. The head might also look comparatively wide.
- Metopic Suture: The brow can’t grow in width so looks very pointed and narrow. The eyes can look pinched towards the centre of the head.
- Lambdoid Suture: This is the most rare of the craniosynostoses and is very seldom seen. This is the one which looks most like a deformational plagiocephaly. The ear on the affected side is pulled back towards the suture, there can be a high bulge on the opposite side of the synostosis and a low bulge below the ear on the affected side.
Craniosynostosis treatments
Surgical intervention is the primary approach to correct craniosynostosis. Two distinct surgical methods are employed, with monitoring extending up to 18 to 24 months of age. During this period, if surgery is deemed necessary, a craniofacial surgeon will undertake a procedure to remodel the upper part of the skull. Such surgical remodeling is also planned if the infant has a genetic syndrome, as part of their comprehensive treatment plan.
More recently, endoscopic surgery has gained prominence and is increasingly offered, especially in the UK. Typically performed on infants under 4 months old, this method boasts reduced invasiveness, minimal blood loss, shorter operation times, and briefer hospital stays post-surgery. The procedure involves inserting a camera beneath the skin, allowing the surgeon to open or completely remove the fused suture. This intervention enables the skull to naturally remodel as the infant continues to grow. Subsequent to surgery, a scan photograph of the infant’s head is taken, and a custom-made helmet is fashioned. This specialised helmet facilitates the gradual restoration of the head’s normal shape over the ensuing months.
Known as Endoscopic Suturectomy with Postoperative Helmeting (ESCH), this approach is recognised for its reduced impact on the infant and its promising outcomes.
Technology in Motion collaborates closely with Great Ormond Street Hospital to provide cranial helmets, aiding infants after cranial surgery. Feel free to reach out for an in-depth discussion about treatment options. at info@technologyinmotion.com, or call 0330 100 1800. Alternatively, you can send us an enquiry.
For more information access our comprehensive craniosynostosis guide.





